
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*, Wai Yung and Carlos Eduardo Sabrosa
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: December 21, 2025 ; Revised: December 23, 2025 ; Accepted: December 25, 2025 ; Available Online: January 01, 2026
Citation: Millstein PL, Yung W & Sabrosa CE. (2025) The Clinical Affect of Occlusal Contact on Implant Restorations. J Oral Health Dent Res, 5(2): 1-3.
Copyrights: ©2025 Millstein PL, Yung W & Sabrosa CE. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
This paper describes a method to record and classify profiles of occlusal contacts.
The anatomy of occlusal contacts and contact areas can be used in the design of implant prostheses.
Keywords: Occlusal contact. Imaging, implant hardness, ceramic restoration, force distribution.
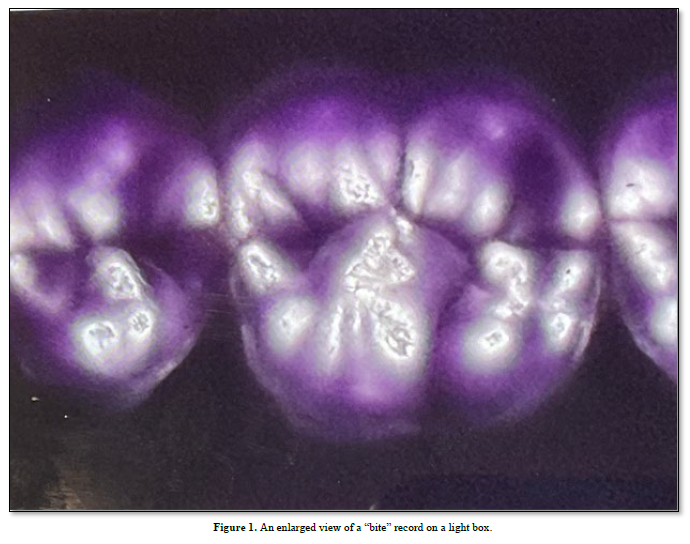
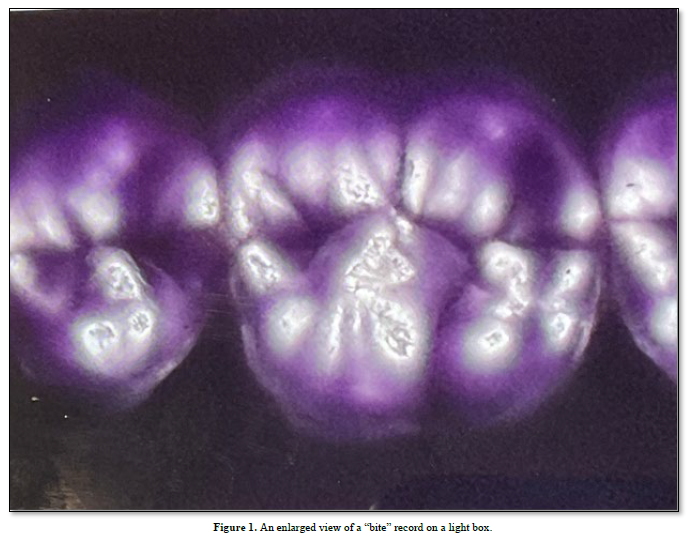
A definition of force is “an influence to change the motion of a body or produce motion or stress in a stationary body” (1). It can be described as a destructive element when an object propelled by a forceful thrust fracture, upon impact, an opposing object. Intensity of force increases with the forced movement of an anchored object (2). Force is used to move objects; intensity of force can break or bend them such as with teeth and crown restorations. The impact of opposing teeth and the force applied upon closure may be described as natural if the teeth function in harmony (3). Force distribution will be even. If the force distribution is uneven then impact upon closure may contribute to a poorly functioning occlusion. Intensity of occlusal contact occurs in any resistant area of a working occlusion. Tooth grinding, tooth and crown breakage, TMJ pain, and general malaise are often attributed to an unbalanced and maladaptive occlusion. A patient cannot treat an uneven bite by self-imposed tooth grinding (4). Uneven force distribution and contact intensity should be treated by a skilled clinician. We record occlusal contacts in conventional bite impressions (5). Contacts are then identified and classified by using image analysis. Searching for ideally placed occlusal contacts with matching cusp fossa designs is misleading because they are non-existent. Intense areas of contact are clearly visible and can be identified (6). Bite force and occlusal patterns are unique for each individual. Bite force can be measured using a force gage. The maximum bite force for a human is 160 pounds per square inch. In comparison over 4000 pounds per square inch was measured in the now extinct Megalodon shark (7). Force is a destructive element when occlusal contacts are not balanced. Resultant tooth damage increases with self-inflicted tooth grinding and bruxism. At present there is no way to record occlusal contact imbalance. The usual dental visit does not include an occlusal exam other than visual identification of Angles’ orthodontic classifications of jaw positions. Using an imaging system a clinician can see and categorize occlusal contact and non-contact areas of the occlusion (Figure 1). Training is necessary to learn how to make a suitable occlusal impression and to interpret the findings. A non-set impression material that is used to record the bite can also be used to make immediate repetitive bite recordings. No two repetitive bites are exactly the same as are no two rhythmical beats of one’s pulse. If recordings of the bite are not repetitive then the results from the recordings will remain in question. Attention to detail when taking impressions is necessary to obtain accurate records. Zirconia crowns are hard and unyielding. Implants are rigid posts. Differences in the mechanical properties of restorative materials makes the intensity of force driven vectors a factor when designing and constructing an implant restoration. If some restorative units bend, and others do not then a compensatory occlusal design must be incorporated into the manufacture of the restoration. Image analysis can be used to avoid incorporating areas of intense contact.
Designing and implementing a balanced occlusion is possible but knowledge of the properties of the restorative materials must be included in the design. Stored data at the time of manufacture and insertion provides essential information for future assessments.
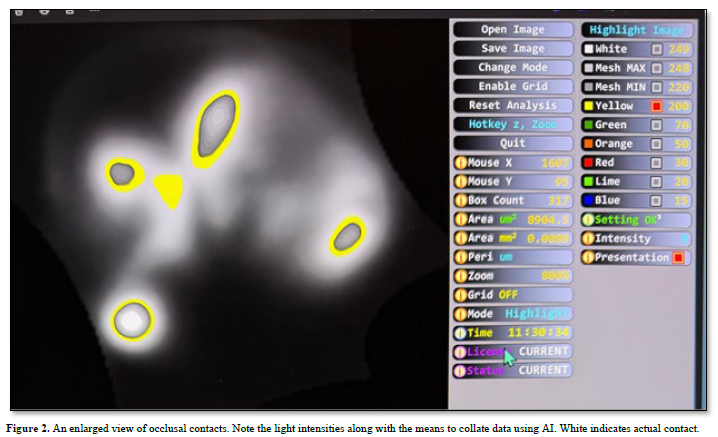
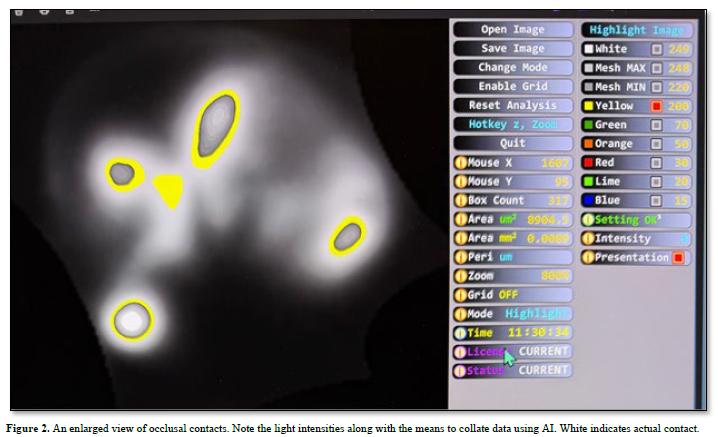
The camera takes the picture and Image analysis provides a means to view and analyze it. The program is housed in an apparatus that consists of a DC light box upon which the sample is placed, a camera which is supported six inches above the box in a black housing, an image analysis program (Image J), and a computer. All images are shown on the computer screen. Images from the impression are formulated from numbers which translate into black and white pictures or converted into associated colors.
Areas can be isolated and further examined (WY). Area content along with light intensity measurements as shown represent the anatomy of an occlusal contact (Figure 2). Such information is permanently recorded. Systems that monitor dental occlusion are scarce. The current use of force sensors in pliant occlusal wafers does not address occlusal contact areas. An occlusal profile of the occlusal anatomy along with contact intensity is not addressed. Anatomy and contact intensities are essential elements in the design of implant restorations. Occlusal repair and early diagnosis of malfunction are assessed by studying occlusal contacts and their associated wear patterns. At present the only way to do this is by analyzing bite registrations using an image analysis program. Permanent records can be used as a baseline for comparison with present day findings. Maintaining good health is the ultimate goal of restorative dentistry.

No Files Found




Internationally Accepted
Share Your Publication :